Light Chain Disorders Indicative of Immune Disorders and/or Cancers Associated with the COVID-19 Infections and Injections- R. Chandler, MD MBA
After being targeted by LNP/mRNA, B- Lymphocytes sometimes malfunction.


Presentation to Doctors for Covid Ethics 1 hour 14 minutes
https://rumble.com/embed/v6y2soi/?pub=
Presentation Slide Deck Download (below)
The Light Chain Signal: Understanding Immune and Hematologic Change After COVID-19 Infection and Vaccination
Our immune system depends on white blood cells called B lymphocytes, or B-cells, which manufacture the antibodies that recognize and neutralize viruses, bacteria, and other foreign particles. Every antibody molecule is built from two types of building blocks: heavy chains and light chains. When B-cells become highly active—such as during infection, inflammation, or vaccination—they produce an enormous surplus of these light chains. Only part of this output is used to assemble complete antibodies; the rest circulates freely in the bloodstream as serum free light chains (sFLCs).
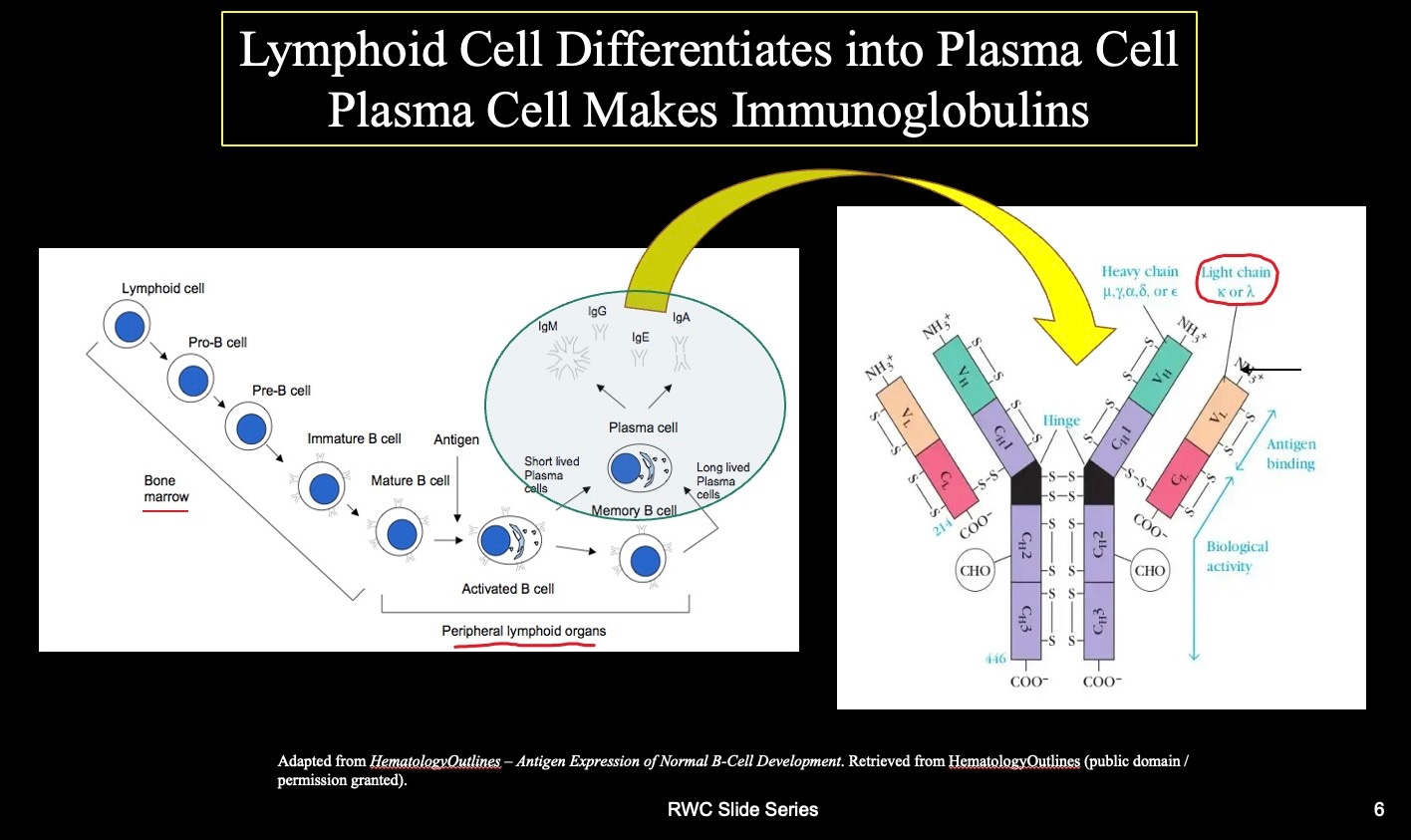
Figure 1: Differentiation of B-cell lymphocytes from hematopoietic stem cells into plasma cells that produce antibodies in response to foreign proteins.
These free light chains are normally harmless and are cleared from the body through the kidneys within a few hours. However, when the immune system is persistently stimulated or becomes unbalanced, sFLC levels can rise sharply. Because they respond so quickly to changes in immune activity, they are among the most sensitive biomarkers of B-cell behavior. Clinicians already use them to detect early signs of plasma-cell and lymphoid disorders such as multiple myeloma, amyloidosis, and monoclonal gammopathy of undetermined significance (MGUS)—conditions where a single clone of B-cells grows abnormally.
In this study, published in the International Journal of Vaccine Theory, Practice, and Research (IJVTPR, 2025), unusual patterns of sFLCs reveal hidden immune or hematologic disturbances after COVID-19 infection or mRNA vaccination. By comparing data from the Vaccine Adverse Event Reporting System (VAERS) and from published clinical studies, the work outlines a clear hierarchy of immune activation—from mild infection to severe disease and post-vaccination reactions—and explores how these patterns may connect to longer-term immune or hematologic changes.
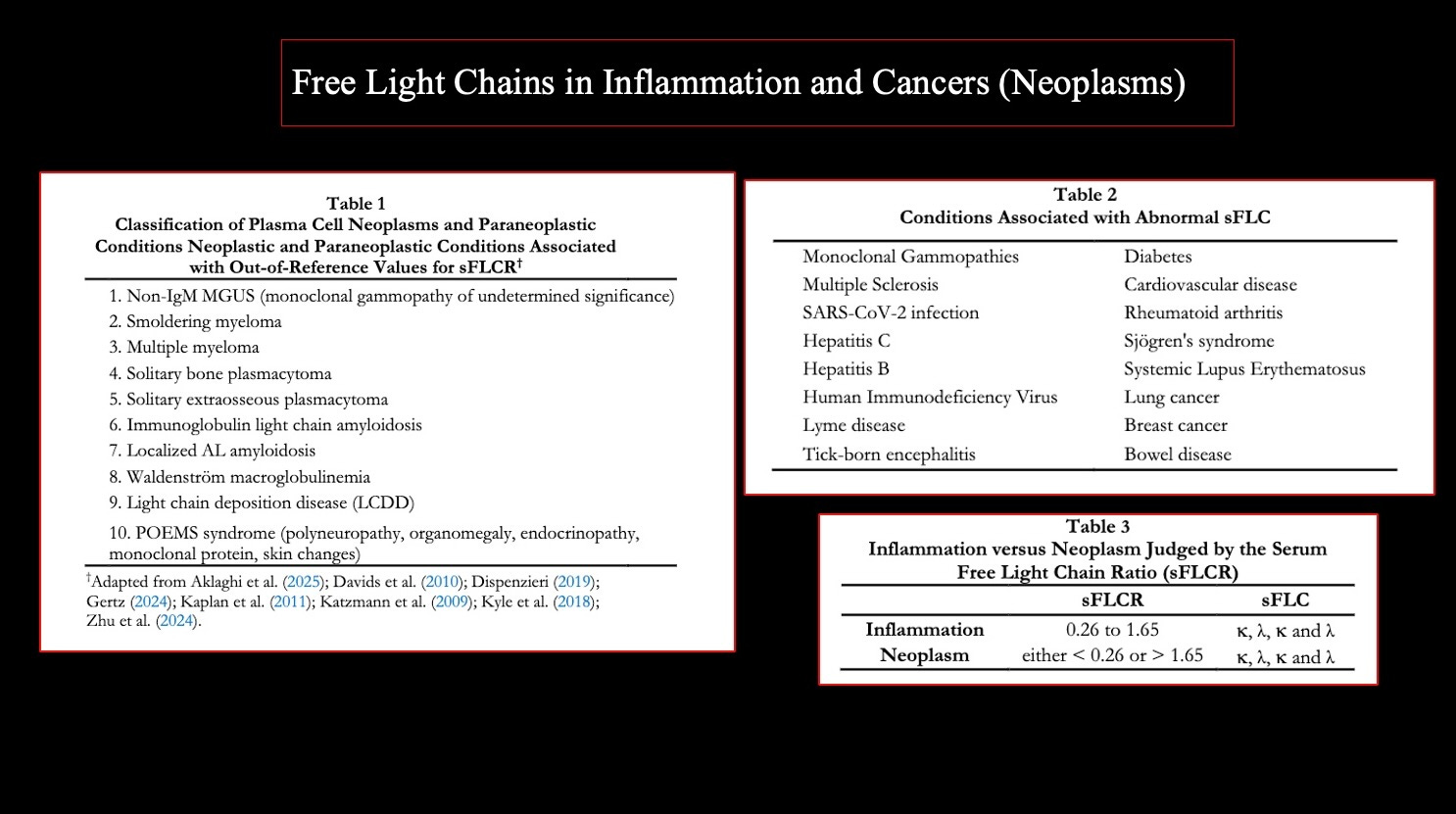
Figure 2: Free light chain elevations in blood cancer cases (Table 1), other conditions (Table 2) and k/l ratios differentiating inflammatory from cancerous conditions (Table 3).
1. What Are Free Light Chains?
Antibodies (immunoglobulins) are composed of two heavy and two light chains, joined in a Y-shaped structure. The light chains—kappa (κ) and lambda (λ)—are produced in excess by B-cells and plasma cells. Unbound chains enter the bloodstream as serum free light chains (sFLCs) and are rapidly cleared by the kidneys.
In healthy adults:
- κ (kappa) half-life ≈ 2–4 hours
- λ (lambda) half-life ≈ 4–6 hours
- Normal κ/λ ratio ≈ 0.6–1.65
Because of their short half-lives, sFLCs are sensitive indicators of real-time B-cell activation and antibody synthesis. Increased concentrations signal heightened immune activity, inflammation, or early plasma-cell proliferation.
Renal function strongly influences sFLC concentrations. κ chains, which are smaller and filtered faster, rise disproportionately when kidney function is impaired. Ratios and ranges must therefore be interpreted alongside renal indices such as eGFR and serum creatinine.
2. The Hierarchy of Changes in COVID-19 and Vaccination
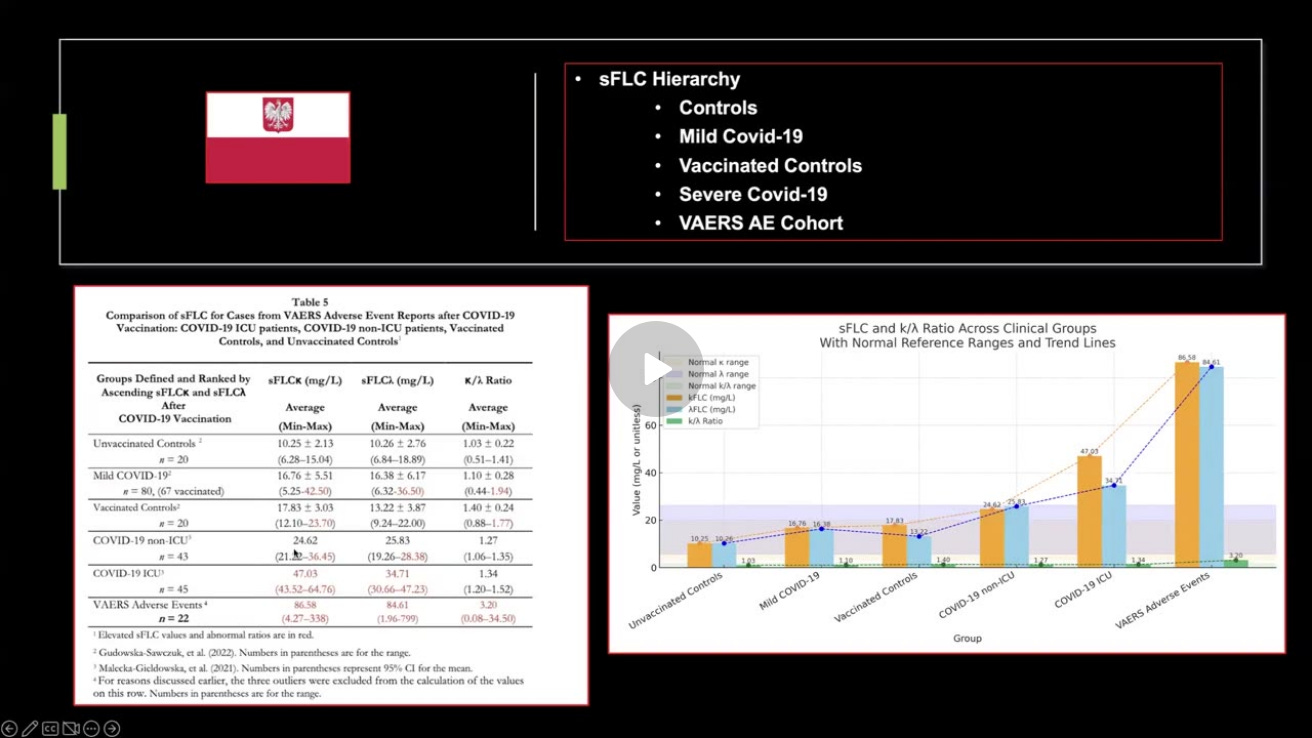
Infection with SARS-CoV-2 and subsequent vaccination both stimulate B-cell proliferation. Studies from Gudowska-Sawczuk and Małecka-Giełdowska (2021–2022) established that even mild COVID-19 elevates both κ and λ light chains above normal. The IJVTPR study extended this work, introducing a comparative hierarchy that ranks immune activation across five clinical groups:
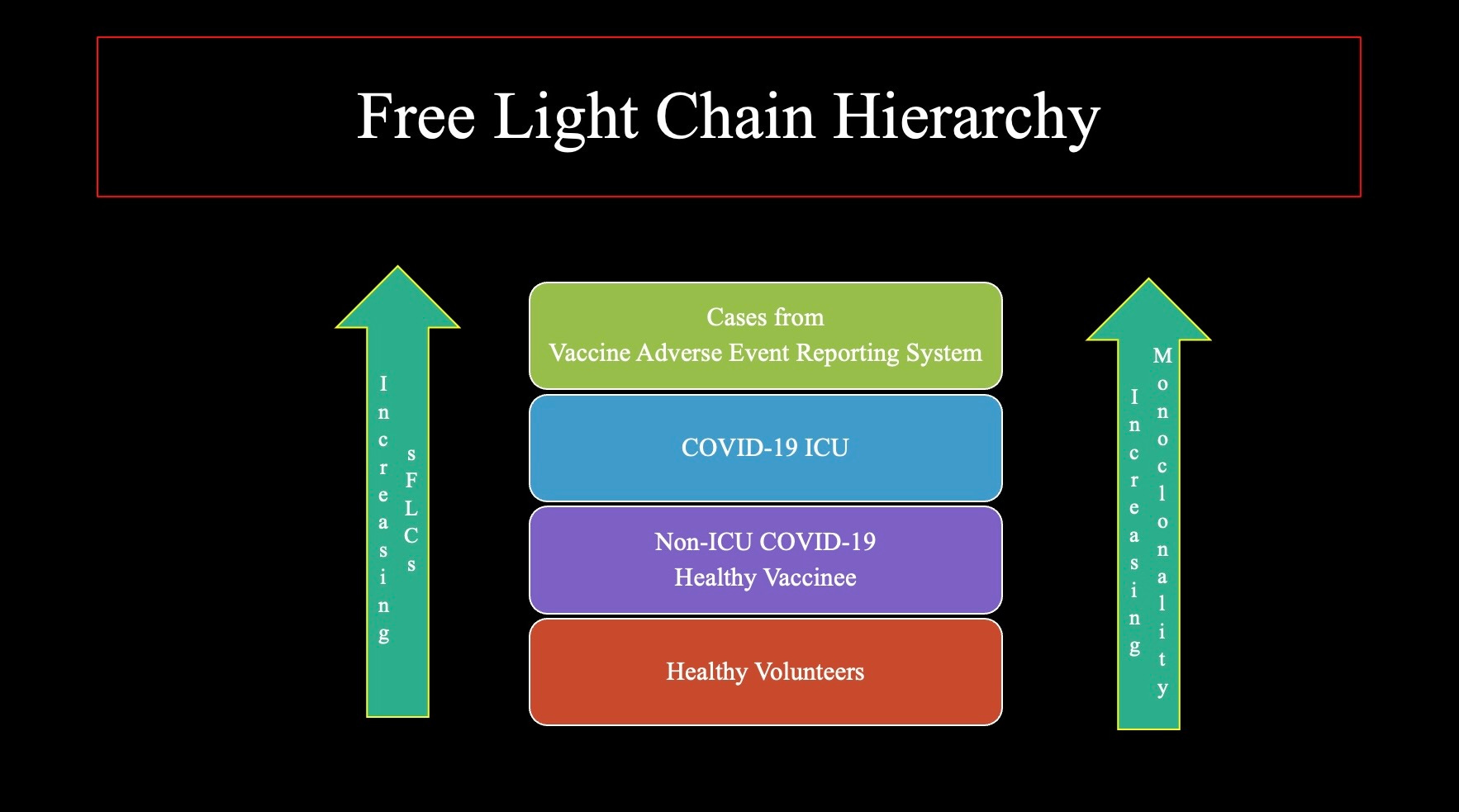
Figure 3: The top level, the adverse event cohort from VAERS, demonstrates elevated ranges for light chains and out of reference range values for the ratio between kappa and lambda marking a shift from inflammatory to cancerous response.
Average findings (mg/L):
· VAERS Adverse-Event Cohort – κ 86.6 / λ 84.6 (ratio 3.20)
· COVID-19 ICU – κ 47.0 / λ 34.7 (ratio 1.34)
· COVID-19 non-ICU – κ 24.6 / λ 25.8 (ratio 1.27)
· Vaccinated Controls – κ 17.8 / λ 13.2 (ratio 1.40)
· Mild COVID-19 – κ 16.8 / λ 16.4 (ratio 1.10)
· Unvaccinated Controls – κ 10.3 / λ 10.3 (ratio 1.03)
This pattern reflects a progressive shift from physiologic immune activation (infection or vaccination) toward pathological over-activation or dysregulation (persistent immune drive and potential neoplastic change). Video link below.
The data reported in the IJVTPR article for the VAERS cohort illustrates the shift from inflammatory values to neoplastic values as shown below in Figure 4. The area between the diagonal lines signifies a normal ratio or polyclonal (inflammatory) response to those outside of this area indicating a shift to monoclonal or cancerous response.
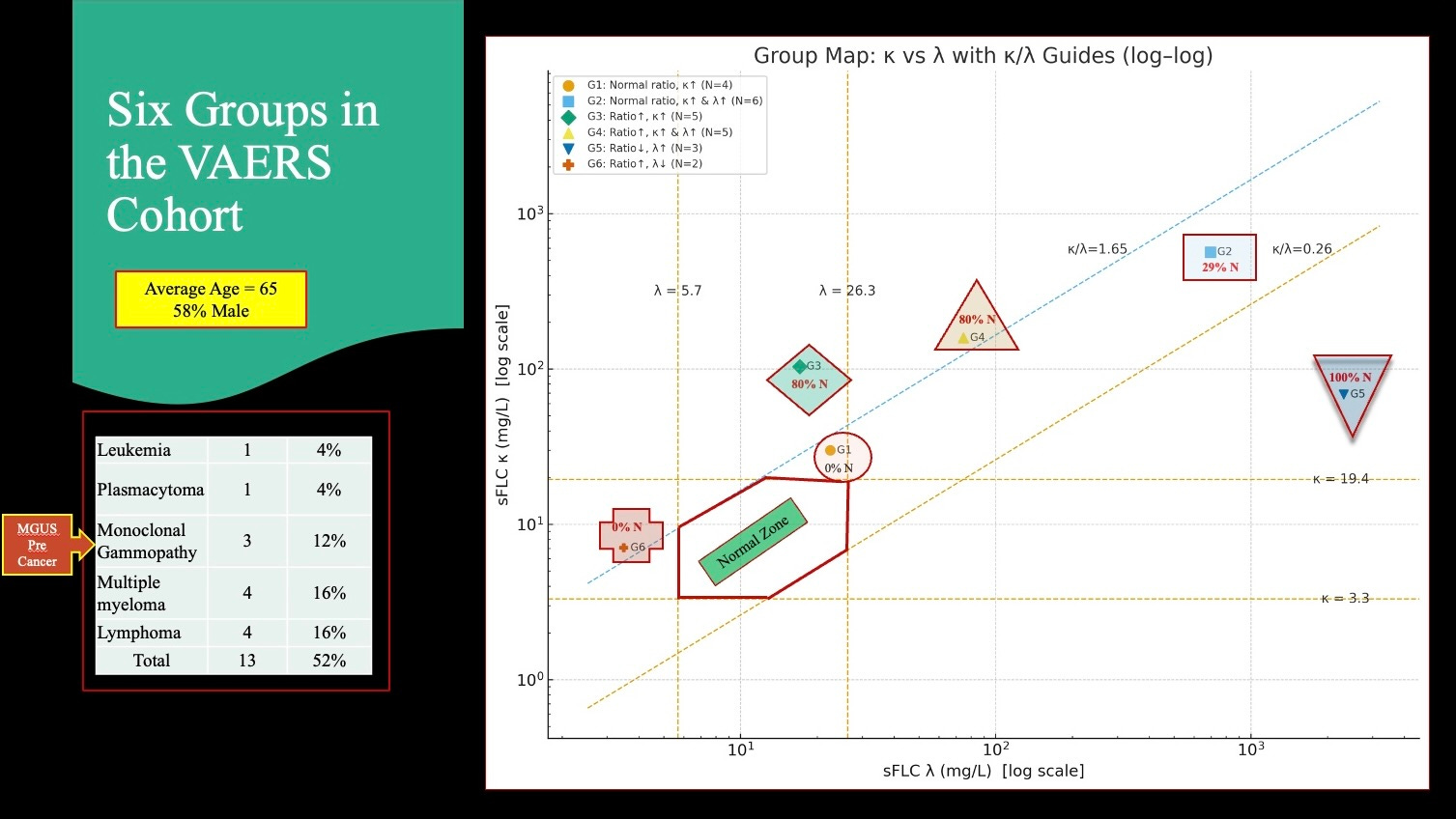
Figure 4: Log Log plot of VAERS cohort data showing a monoclonal pattern with out of reference range values for k/l ratios. Note the high percentage of cancers in these three subgroups. The anomaly is the Cross at the lower left in which there is no elevation of k or l but rather a drop below normal values for l suggesting suppression of lambda producing plasma cells.
3. Pathological Correlates and Tissue Findings
Histopathological examinations described by Burkhardt et al. (2024) demonstrate lymphocytic aggregates in multiple organs, including spleen and lung, forming tertiary lymphoid-like structures (TLS).
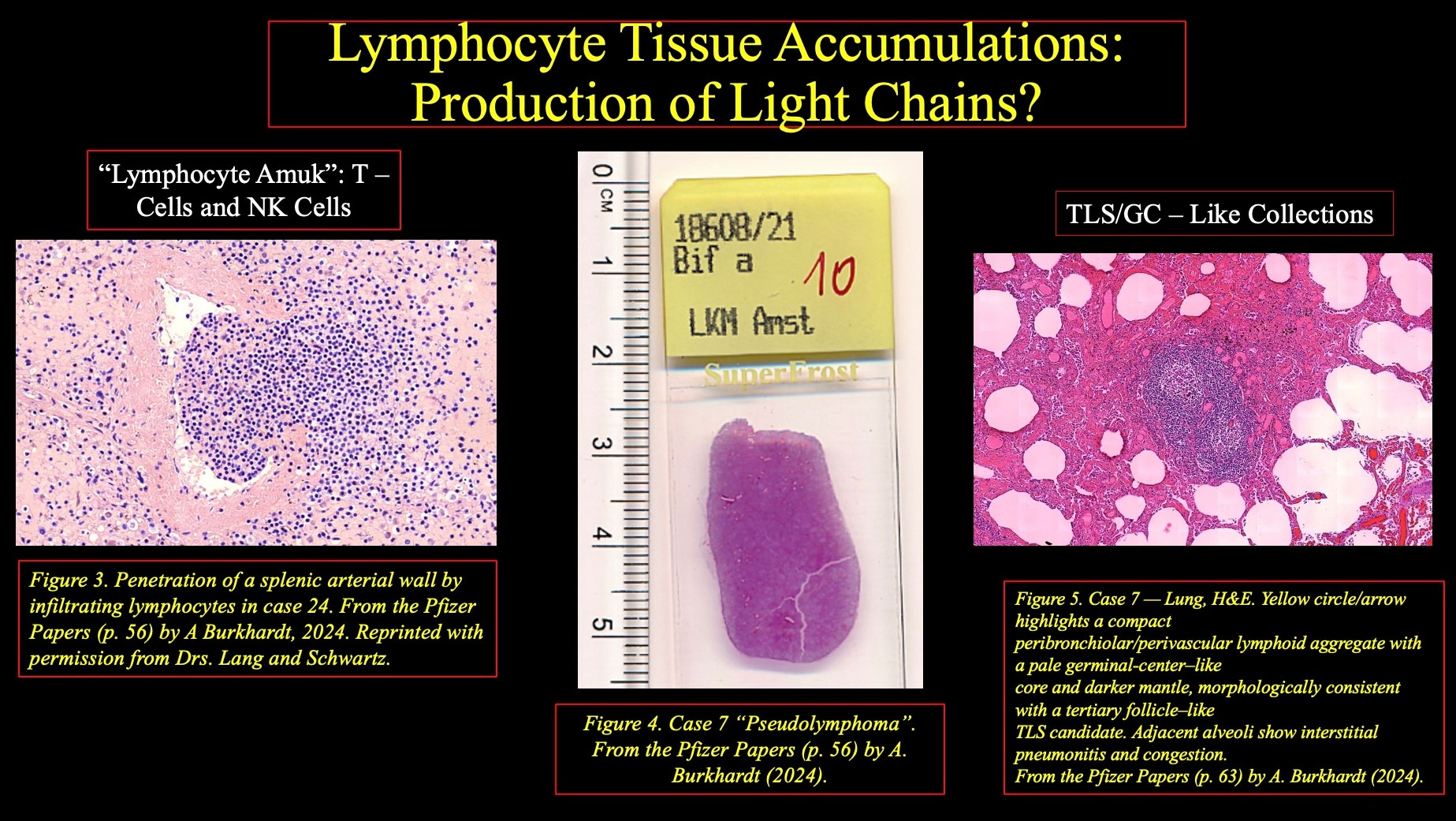
Figure 5: Histopathological analysis from the Burkhardt/Lang Collection show lymphocyte mediated tissue destruction and lymphocyte accumulations resembling lymph node-like structures in various non-lymphoid organs.
These structures potentially act as localized immunoglobulin production sites, a possible explanation for sustained Free Light Chain elevations in some people.
4. Integrating Clinical and Biomarker Evidence
These findings align with independent reports from Semmler (2022) and Mundorf (2023) showing persistent inflammatory biomarkers in post-vaccination fatigue syndromes.
A search of the VAERS database reveals a clear signal for B-cell malignances following COVID-19 vaccination with 4.4x the number of reports for all other vaccines administered from 1990 to 2025. Figure 6 below shows the top 20 B-cell malignancies and which vaccine type they followed.
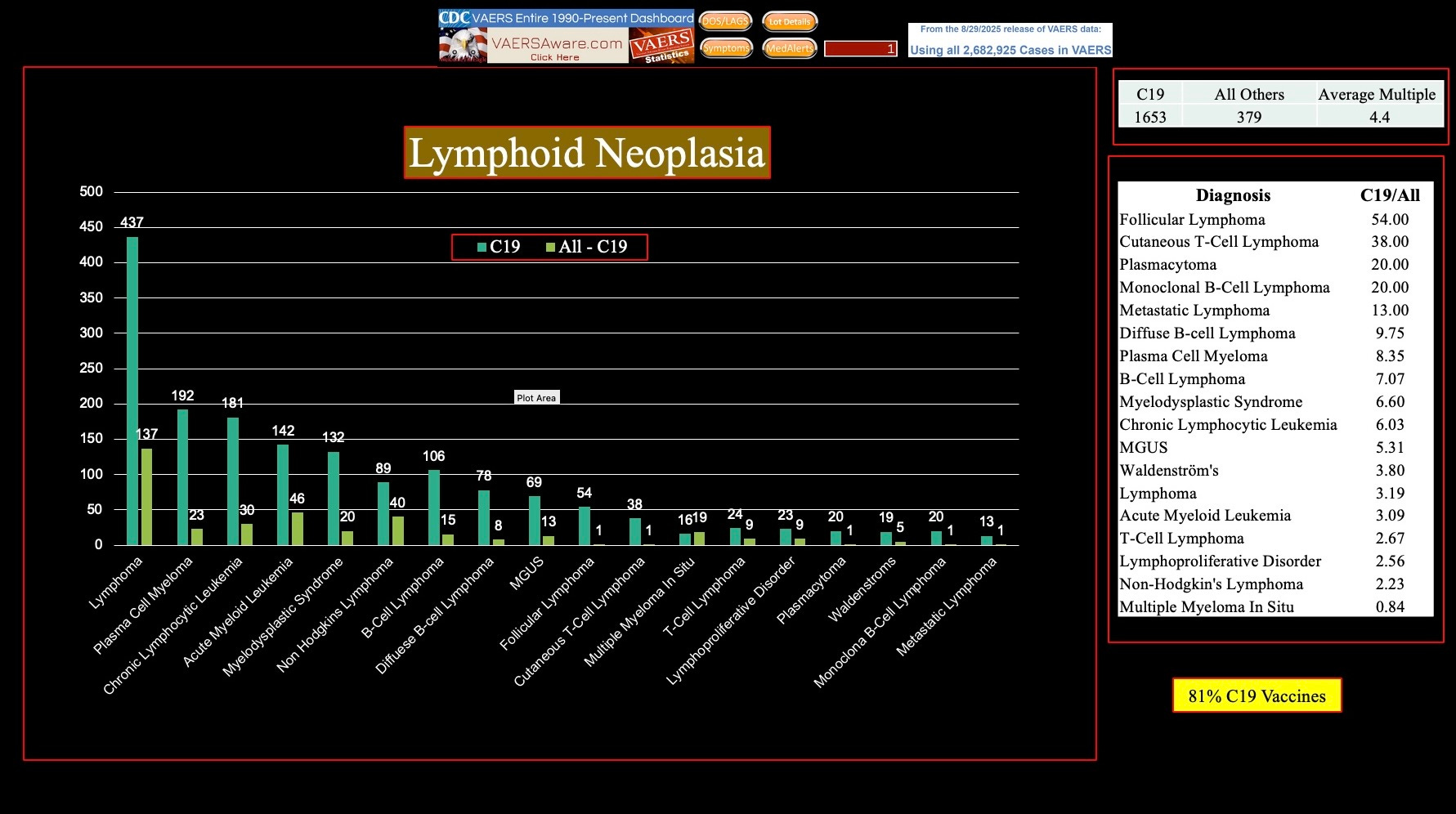
Figure 6: 81% of Mature B-cell cancers reported in VAERS follow COVID-19 vaccination, a 4.4 fold increase compared with all other vaccines from 1990 to present.
Miki, et al. reported a spike in deaths from Myeloid (non-lymphocyte) blood cancers suggesting LNP/mRNA adversely affects Myeloid as well as Lymphoid cells.
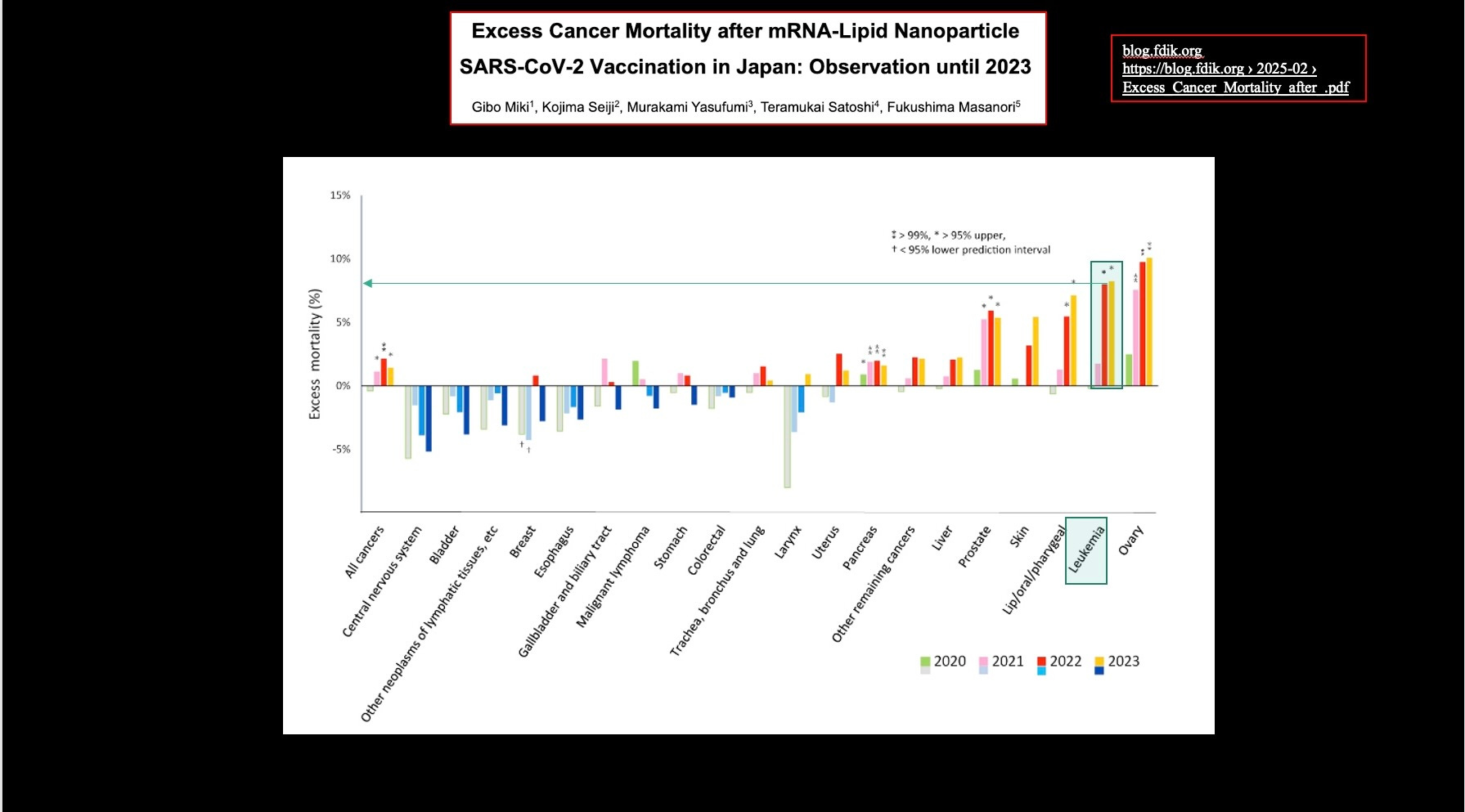
Figure 7: Real world data from Japan show another type of blood cell cancer, leukemia, has spiked up following introduction of COVID-19 vaccine products. Japan is a high compliance country with almost 100% vaccinated, some with as many as 10 doses.
5. Conclusions and Clinical Implications
1.Prolonged immunological response to COVID-19 vaccination has been established by unique profiles of biomarkers, clinical disease clusters, destructive lymphocyte mediated histological and immunohistochemical findings.
2.Systematic linkage of biomarker profiles and clinical clusters to patterns of organ-specific and unique pathological findings under a unified concept from COVID-19 vaccination is a logical next step. CoVax Disease is proposed as a unifying concept for distinct disease clusters following COVID-19 vaccination.
3.Measurable increases in serum free light chains (sFLCs), particularly sFLCs as a marker of B-cell activation, have been demonstrated for SARS-CoV-2 infection and mRNA COVID-19 vaccines.
4.Inflammatory responses as measured by traditional biomarkers like IL-6 accompany polyclonal elevations with normal sFLCR.
5.A subset of cases reporting post-vaccination adverse events to VAERS have monoclonal gammopathies, including elevated sFLC kappa/lambda ratios, extremely high absolute FLC values, and, in some cases, clinical diagnoses of MGUS (Monoclonal Gammopathy of Undetermined Significance), multiple myeloma, or amyloidosis.
6.Vaccination with mRNA COVID-19 injectables may induce or accelerate underlying plasma cell disorders in some individuals.
7.Physicians should work up and monitor patients with out-of-range sFLC values, even when sFLCRs are within the reference range, as a spectrum of related medical conditions may emerge.